You just have received endorsement from the outgoing nurse. You check on the chart and assess your patient. You check the IV lines and IV sites, you check the due medications and if the stock’s enough for the 8-hour shift. You check when the IVF’s will be due. You check the vital signs then record it. All within normal range.
Everything was just doing fine. Today is going to be a non-toxic duty, you say to yourself, until…
“Nurse,” the nursing attendant calls you.
“The patient does not have urine output for this hour”
“Really?” you sound surprised. Just a while ago, you thought no problem would arise.
“Okay, I’ll just check again after a few minutes”
“Okay”
After a while, still no urine output. You check the tubings, “Uh-oh, what’s this? I think it’s all clogged up”
You note the presence of blood clots in your catheter tubings. Now you know the culprit, but what should you do?
 Cystoclysis: An overview
Cystoclysis: An overview
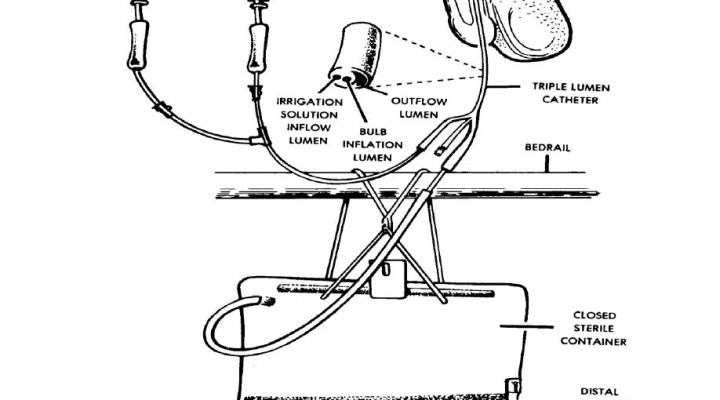
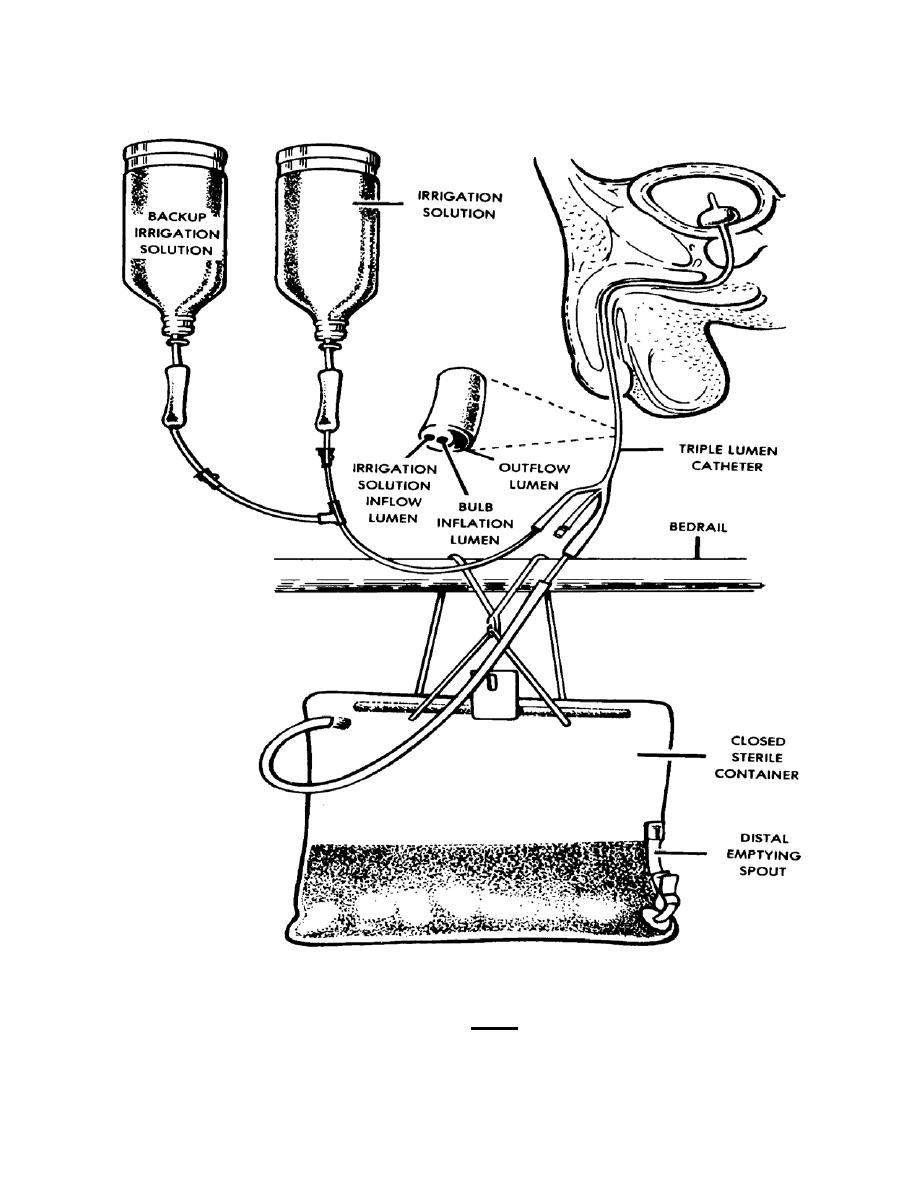
Cystoclysis or bladder irrigation may be defined as the process of flushing the bladder with normal saline continuously to prevent or treat clot formation, allowing urine to flow freely and maintain IDC patency. Here, a special catheter is used. It may also be used to instill medications such as antibiotics for treating bladder infections, is done over a period of time, and runs continuously.
Other purposes of bladder irrigation includes relieving bladder spasms as draining urine from the bladder can relieve spasm; wash out any residue urine or sediment; prevent formation of calcific deposits in and around the indwelling catheter; and to drain the bladder when acute urinary retention is present. However, like any other invasive procedure, cystoclysis must be performed aseptically so as to prevent infection.
Usually, this is indicated for patients with Urinary Tract Infection, post-genitourinary surgery, prostatic hematuria, urinary retention, and for patients who had undergone prostatectomy.
To perform this procedure, you may need:
- 3 way catheter
- 9% sodium chloride irrigation bags as per facility policy
- continuous bladder irrigation set and closed urinary drainage bag with anti-reflux valve
- Chlorhexidane 0.5% with 70% alcohol wipes
- Non sterile gloves
- Personal protective equipment
- Underpad (bluey)
- IV pole
Nurse’s Role
As nurses participating in this intervention, we must always be aware of our responsibilities and role. Prior to the procedure, you must first check the doctor’s order for the type or irrigation and irrigation solution needed. Confirm client’s identity and explain procedure to the client. Make sure that the patient understands it well and you may need to obtain informed consent.
Gather materials and make sure that everything is in order and complete. Then, perform medical handwashing and provide privacy to the patient.
During the procedure aseptic technique must be observed. First you must drape the patient exposing the leg where the catheter is being taped. Then, do gloving and cleanse the catheter injection port with an antiseptic swab. Remember to maintain sterility at all times and make sure that you are only exposing the site.
Swab IDC irrigation and catheter ports with chlorhexidine swabs and allow drying. After that, remove the spigot from the irrigation lumen of the catheter using sterile gauze and discard the spigot. Connect the irrigation set to the irrigation lumen of the catheter still observing the aseptic technique. Then remove the spigot or old drainage bag from the catheter lumen using sterile gauze and apply catheter drainage bag maintaining clean procedure.
Remember not the start bladder irrigation until the urine of the patient is flowing freely. If it is, then you must unclamp the irrigation flask that was used to prime the irrigation set and set the rate of administration by adjusting the roller clamp. Regulate the flow well.
We must ensure that there is adequate supply or irrigants nearby as this procedure may be done continuously and as necessary depending on the degree of the hematuria.
After each flask is complete, empty urine drainage bag and immediately record urine output on the fluid balance chart, before you begin with next irrigation flask. Also, to prevent infection especially those catheter related UTIs, the nurse must ensure that regular catheter care is given and must be documented in the nurse’s notes as well as NCPs.
Not only should you note the amount of urine output, but the nurse must also note the descriptions such as urine color and degree of hematuria, as well as patient’s comfort.
Sources:
- https://nursing-the-nurse.blogspot.com/2010/03/cystoclysis.html
- https://prezi.com/nokyhjrgxiyc/irrigating-cystoclysis/








